
The Health Service Journal has published data (subscription required) detailing the number of patient misidentifications in the NHS. The numbers are staggering.
Responses to Freedom of Information requests from 166 trusts revealed 58,537 cases of patient misidentification logged in Datix or other patient safety systems between 2019 and 2023, including 4,713 causing some sort of harm. This is equivalent to 11,707 incidents a year, with 943 leading to harm.
As with many safety steps in healthcare, checking identification is simultaneously both fundamental and frustrating. Anything that takes time, any barrier that is put in place to prevent error, slows down the way we work, and human nature dictates that short cuts will be found and taken. Indeed, patients themselves can get frustrated with endless reconfirmations.

Interestingly, misidentification was once regarded as a Never Event, entering the list of 25 errors that should never occur in 2012/13, only to be removed 2 years later. Why? Never Events must, ‘Be wholly preventable, where guidance or safety recommendations are available at a national level, that provide strong systemic protective barriers have been implemented by all healthcare providers.’ It seems that the NHS England did not believe that there were sufficient barriers.
The Health Safety Investigation Board (HSIB) published a report on this subject in Feb 2024. It recognised that, ‘patient misidentification is challenging to address and previous efforts to reduce the risk have not been as successful as hoped’. This is clear from the data presented by HSJ. HSIB drew together evidence from the literature and accounts from patients, families and staff provided examples and vignettes which give insights into the challenge.
When a misidentification occurs, there is always a reason. Assuming it is not a blatant lack of engagement by staff, some situational quirk, coincidence, unintentional lapse, distraction, patient specific factor, or unexpected environmental issue will be found.
HSIB refers to specific patient related factors, such as diminished level of consciousness, communication or language barriers, and populations where surnames are particularly common and cannot be used to differentiate individuals. Walk onto any ward and you might notice big red arrows or other marks next to patient names on the board, put there to alert staff that there is a ‘duplicate’; efforts are usually made to physically separate them as well, thus reducing the risk of one being the other’s medicines.
It is easy to see how urgency breaks through such precautions. Imagine Mr J. Smith, suffering from pneumonia. His oxygen level falls critically. His nurse puts out a peri-arrest call. The first member of the crash team arrives, and asks where Mr Smith is. Another nurse points along the ward, to the Mr Smith they know. The doctor finds Mr C. Smith and starts to assess or treat him. Perhaps they perform an arterial blood gas sample. This is now an intervention, not just an assessment.
Patients do not need to have the same name. The case against paediatrician Hadiza Bawa Gaba (see previous posts) was strengthened by her error when called to the ward after Jake Adcock collapsed. Resuscitation had been commenced, but thinking that the patient in a side room was a terminally ill child whom she had seen earlier in the day, and who was ‘not for resuscitation’, Dr Bawa Gaba called the attempt off. It took two minutes for the crash team to recognise the error. A tragic example of an emergency situation breaking down any and every precaution that could be put in place.
The HSIB report includes this comment, from an ambulatory setting: “[It is] amazing how many people … you can call a person by name and not the right person stands up.” This has happened to me. Maybe I was unclear when I called them from the waiting area, or maybe the (wrong) patient’s desire to be seen and their level of internal tension resulted in them jumping up soon as I spoke; most likely, their surname had some similar vowels in it. They followed me back to the clinic room and I happily started the consultation with the right patient’s details in front of me on the screen and the wrong patient in the chair. They looked blank but not particularly concerned when I asked about their liver disease. It took over five minutes for us both to realise that we had made a mistake. Why did they not say, “Doctor, I have none of these problems!” It is easy to underestimate how passive patients can become in front of a doctor. The level of trust is great – we must know what are talking about!
An HSIB investigation published in June 2021 describes a very similar incident, but with far more significant consequences.
In July 2019 a woman aged 39 years (Patient A) visited the gynaecology outpatient department for her first fertility treatment appointment. Another woman (Patient B) also attended at a similar time for a colposcopy appointment. At the reception desk they were both checked in and directed to the same waiting area. A nurse entered the waiting area and called out patient B’s first name and surname twice. As the nurse received no response she then called patient B’s first name. Patient A’s surname was similar to patient B’s first name, and, as no other person had responded, Patient A believed the nurse must be calling for her. She was unfamiliar with the nurse’s accent so she sought to clarify that she had understood correctly, by repeating her surname to the nurse. […] Patient A went on to receive a colposcopy procedure and left the outpatient clinic. Patient B then went in for her appointment. The error was quickly identified by staff who telephoned Patient A and asked her to return to the outpatient clinic on the same day, where staff explained what had happened and apologised for the incident. Patient A then had her intended fertility clinic appointment.
For HSIB, checking the NHS number appears to be the great hope. It cannot be confused with another, it is unique. However, it is cumbersome, 10 digits long. In my trust, we do not use it. The hospital number, usually 6 or 7 digits, seems to provide the same degree of safety. An HSIB investigation from 2021 found that one area had ‘adopted a shortcut in using the last four digits of the NHS number to complete the matching task’. A classic short cut.
Finally, HSIB focuses on workload.
Increasing workloads led to staff attempting to be more efficient. This was found to reduce thoroughness – known as the efficiency–thoroughness trade-off (Hollnagel, 2009). There was also an example of where procedures called for reduced thoroughness when the clinical workload was increasing.
Short cuts have been examined in the safety literature. As I said earlier, it is human nature to find them. But in safety critical industries, we must find a way to support staff to do things that feel redundant or excessive in every instance. This requires the action to become ‘second nature’, like handwashing. And just as handwashing between patients is now so habitual that we feel dirty if we don’t (I do anyway), failure to positively identify a patient before interacting with them should make us feel unsafe. Like something is missing. I have written previously about checklists and their implementation. When they are introduced, they can feel excessive, but after a while you feel naked and exposed when they are not done!
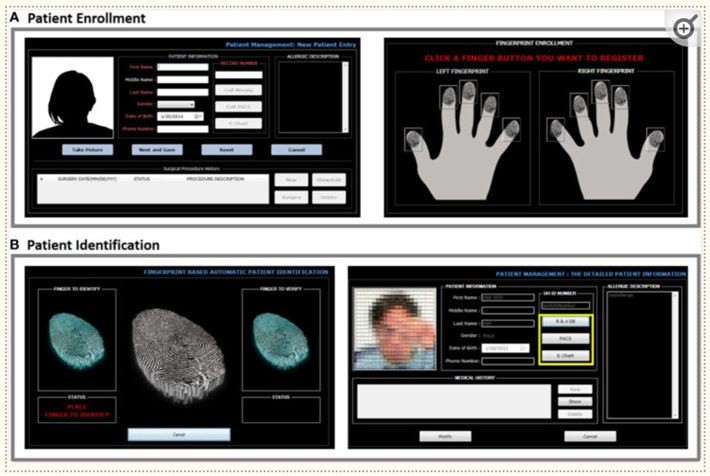
IT and electronic innovations should be able to help. We already have barcodes on wristbands that need to be scanned before giving blood and giving medicines. A large study into the effectiveness of barcodes found that they were not failsafe, with 45,000 errors being made out of 1.7m barcode scans. The next major area of interest is biometrics. Most of us use this with our smartphones and secure apps every day. Medicine is often behind in matters of technology, and there will be concerns about data privacy. However, the ubiquity of electronic patient records and medication charts means that scanning faces, eyes or fingerprints could ‘release’ the relevant chart. Can we imagine patients pressing their fingers onto a pad in clinic, or showing their face to a scanner, in the anaesthetic room, in the ward, before any meaningful medical interaction? Why not? There would be objections. It might feel inhuman. But better than having the wrong operation.
Whatever the future solution, the foundation will always be consistent human behaviour and unfailing attention to detail. This requires concentration, patience (from both staff and patients) and, most importantly, time.
*
Available on Amazon 4.99 paperback, 79p e-book


Leave a comment